川崎症及冠狀動脈病變之B細胞免疫力致病機轉及微菌叢研究
Immunopathogenesis of B cells and microbiota profiles associated with Kawasaki disease and coronary arterial dilation
計畫主持人:臺大醫學系-張鑾英、中研院基因體中心-林國儀
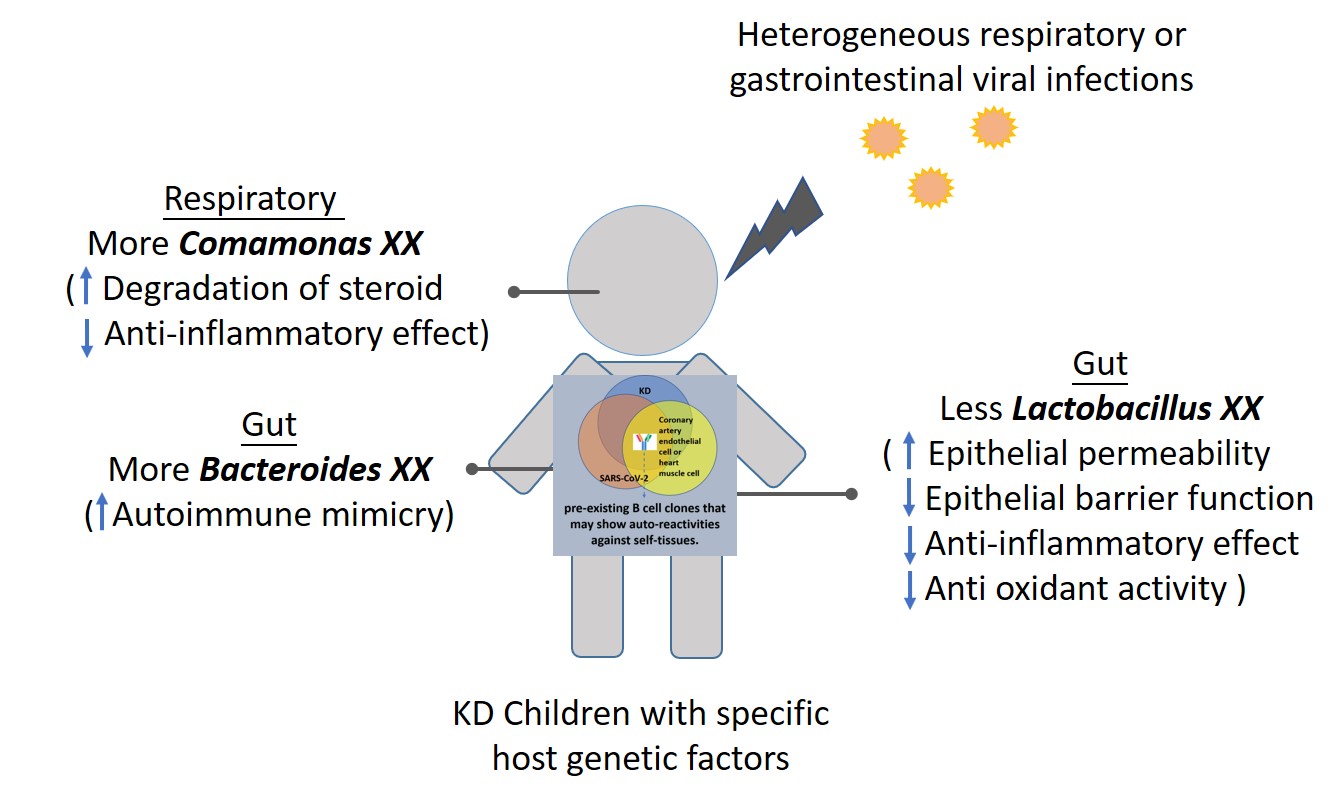
Since the incidence of KD in Taiwan is the third highest in the world and it may have life-threatening disease or possible long-term sequelae of coronary artery, and the appearance of KD-like symptom-multisystem inflammatory syndrome in children (MISC) caused by SARS-CoV-2. KD is very important clinically in Taiwan and worldwide. Our findings demonstrated here suggest the connection of KD and altered gut microbiota, as well as the possible involvement of viral infection in the pathogenesis of KD and COVID-19 via eliciting the activation of certain pre-existing B cell clones that may show auto-reactivities against self-tissues. Through comparisons among patients at different stages of KD and controls, we found that gut microbiome diversity decreased significantly at the acute stage of KD. Compared with the other KD cases without coronary arterial dilatation, KD cases with coronary arterial dilatation/aneurysm also had a lack of lactobacilli. Our results show that the abundance of Rikenella XX in the group with lower B-reg expression (associated with coronary artery lesions) is also lower, indicating the ability of intestinal protection may be insufficient and it is easy to be invaded by pathogens. At the same time, the low expression of B-reg contributed to lower pathogen clearance activity. Both effects may contribute to severe immune response. Dysbiosis and lack of probiotics such as lactobacilli may contribute to the development of KD and subsequent coronary arterial lesions. Through B cell repertoire analysis of the sequences acquired from patients with KD and from SARS-COV-2 infection, we are able to identify several B cell clones from patients with KD that carry similar heavy and light sequences as those from patients recovered from COVID-19 infection. We isolated two monoclonal antibodies from patients with KD that are able to recognize Coronaviruses Spike protein. As KD has maintained its etiology as an enigma, and there is no optimal therapy for refractory KD as well as no preventive way, our findings of B cell repertoire and microbiotas in KD will shed light on understanding of its pathogenesis, potential biomarkers, treatment and preventive approaches.
川崎症在台灣的發病率高居世界第三,如無妥善治療,可能留下冠狀動脈病變後遺症,加上新冠肺炎流行期間,孩童出現類似川崎症全身性血管發炎症狀,因此投入川崎症研究在臨床上是非常重要的。我們的研究結果闡明川崎症與腸道菌相改變有關,以及病毒感染可能透過激活某些先前就已存在的可能有自身免疫反應的B 細胞,透過對抗自身組織,導致川崎症。藉由比較川崎症不同階段的患者和對照組,我們發現腸道菌相多樣性在川崎症急性期顯著下降。。有冠狀動脈擴張/動脈瘤的川崎症也缺乏乳酸菌。也觀察到B-reg表達較低(與冠狀動脈病變相關)組別中,Rikenella XX的豐度也較低,Rikenellaceae在腸道菌相形成的早期與乳酸菌一起發揮保護腸道的作用,RikenellaXX隸屬Rikenellaceae之下,當此菌減少,可能腸道保護能力不足,容易被病原體侵入,同時,B-reg 的低表達導致病原體清除活性降低,以上都可能導致嚴重免疫反應。綜合以上,菌相失調和缺乏乳酸桿菌可能導致川崎症發展和隨後的冠狀動脈病變。經由分析川崎症患者和感染過新型冠狀病毒病人的B細胞組譜序列,我們發現川崎症患者和感染過新型冠狀肺炎的康復者體內的某些B細胞株攜帶相似的重鏈和輕鏈。進一步的實驗結果也顯示,從川崎症患者分離出的兩株單株抗體能辨識冠狀病毒的棘蛋白。由於川崎症的病因一直是個謎,對川崎症中 B 細胞庫和菌相的發現將有助於理解其發病機制、潛在生物標誌、治療和預防措施。